Sunday, November 26, 2023—12:00 pm 37˚F (3˚C)—Light flurries
Hope you all had a Happy Thanksgiving. Great weekend for the Michigan football fans with a three-peat win over Ohio State! Go Blue all the way!
Sumi is slowly changing and has entered a new phase. She is under In-home Hospice Care as of November 16.
This is a big change but nothing that should drastically alter her medical care, safety, well-being and lifespan.
Knowing that the loved ones of some of the caregivers in our support group are in Hospice Care, I was pondering if Sumi would qualify for Hospice Care. And if she does, would it be a good idea to have her in Hospice Care?
On November 7, I reached out to Hospice of Michigan (HoM), a non-profit Hospice service provider, to see if Sumi would qualify. They sent a nurse to our home for Sumi’s evaluation on November 10. The nurse had obtained Sumi’s medical records from her primary care physician (PCP) and based on the history of Sumi’s Alzheimer’s disease, which is considered terminal, Sumi got qualified.
In the eyes of nature, we all are on the path of being terminal at some point. Isn’t it ironic that in Medicare’s eyes, when the path is known it is considered terminal, and the unknown path — non-terminal?
Things were moving fast. For me it was a surprise that Sumi qualified for Hospice Care. As Sumi’s guardian and having DPOA (Durable Power of Attorney) it was up to me to decide if this was the right time for Sumi to enter Hospice Care. I was not prepared to make a quick decision and told the Hospice nurse I needed more time. I wanted to investigate another alternative to Hospice Care – Palliative Care, and understand their pros and cons. I asked the nurse if she could put me in touch with the Palliative nurse. It so happened that HoM does provide Palliative Care and a Palliative Care nurse called me on November 13.
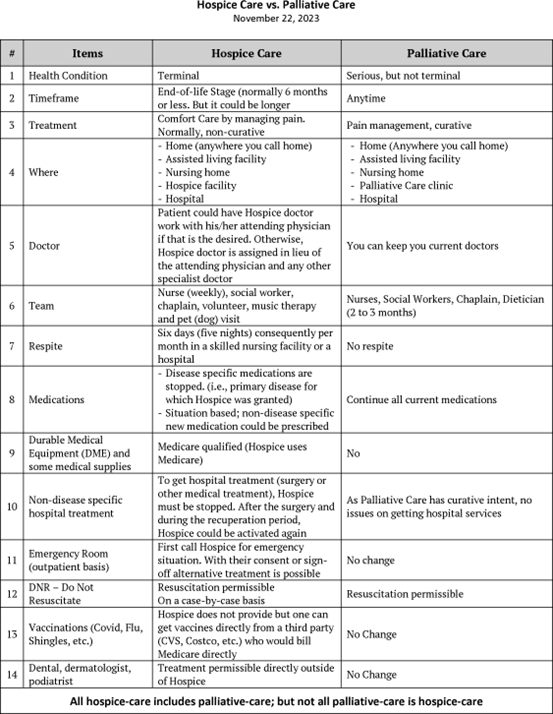
Then I did online research to understand the differences between Hospice and Palliative Care and created a matrix (attached) to compare various items/scenarios of care. I also
got input from Sumi’s PCP, other knowledgeable people who are in the aging field and my caregiver friends whose loved ones are under Hospice Care. Since all hospice is palliative but all palliative is not hospice, the unanimous recommendation was to put Sumi under Hospice Care. Hence, Sumi is in Hospice Care from November 16.
The significant differences between Hospice and Palliative Care are:
- Hospice is non-curative meaning all medications for the disease for which Hospice Care is given need to be stopped. As Sumi is not on any medication for Alzheimer’s, or any other medical conditions, this was a moot point. Palliative Care is curative.
- The Hospice doctor, nurse and social worker would take over Sumi’s treatment from Sumi’s primary care physician and her neurologist. Again, as Sumi is not under any active medical care from her PCP or neurologist, I reasoned it would be okay for the Hospice doctor and nurse to be responsible for Sumi’s medical needs. In Palliate Care, you retain your current doctors.
- For the family member’s well-being, Hospice provides respite care for six consecutive days (five nights) per month in a nursing facility of HoM’s choosing. A chaplain is also assigned for emotional and spiritual support. Palliative Care does not provide respite. Hospice Care has many stigmas and negative connotations. For most people, it is considered an “end-of-life” stage or when people are “actively dying.” Many myths surround it, and from my research, I found:
- Myth #1: Hospice is just for cancer. It is not. It is also for dementia, heart disease, COPD (Chronic Obstructive Pulmonary Disease) or other terminal conditions.
- Myth #2: Hospice is a “death sentence.” On the contrary, the support of Hospice Care can help people live longer.
- Myth #3: Under Hospice, you lose autonomy of care. Not at all. An important point that helped me make my decision is the flexibility of managing Sumi’s care by allowing us choices with self-determination and empowerment. I can have Sumi opt out of Hospice Care whenever I want and have her re-admitted to Hospice Care with recertification.
- Myth #4: Hospice Care costs extra. It is an already paid-through-taxes, Medicare health care benefit that covers services such as Durable Medical Equipment (wheelchair, hospital bed, Hoyer-lift, Broda chair and so on), medications, some medical supplies, respite and volunteer care.
Based on all of the above, I reasoned that starting Hospice Care sooner was a prudent step. If Sumi’s destiny is to have a certain lifespan based on her physical, emotional, mental and brain health due to Alzheimer’s, having her on Hospice should not have any impact on her longevity – her death is not hastened or delayed and nature is allowed to take its course in the comfort of our home without pain or suffering.
In short, in addition to Sumi’s current caregivers, I am getting another layer of 24/7 on- call comfort care and support for Sumi and new connections and emotional support for me thorough the Hospice Care team. We already had home visits from a case manager nurse every week and a social worker who visits every two weeks. A chaplain is scheduled to visit next week.
Time will tell how the decisions made now will affect Sumi’s future care and comfort.